
Australia’s home care providers are being asked to do more than ever: respond faster, coordinate broader services, meet higher expectations for transparency, and keep clients safe while navigating workforce shortages and tighter governance demands.
At the same time, the operating environment has changed. The Australian Government’s Support at Home program replaced Home Care Packages and Short-Term Restorative Care from 1 November 2025, with the Commonwealth Home Support Programme (CHSP) transitioning no earlier than 1 July 2027. This shift puts even more emphasis on clear service information, service agreements, and consistent delivery across an increasingly complex care landscape.
If you’re a provider aiming to scale more clients, more services, more regions – your biggest constraint often isn’t demand. It’s coordination. And that’s exactly where a purpose-built client management system (CMS) like a DC2Vue Support at Home Module can become the growth engine: standardising operations, reducing admin drag, improving compliance, and giving leaders real-time visibility into service delivery and outcomes.
The Scaling Trap: When Growth Creates Chaos (Now With Brokerage + POS + Invoice Matching)
Many providers start with a strong care team and good intentions, then hit a familiar wall:
Client onboarding is manual and inconsistent.
Care plans live in documents and emails, not in a system that “drives” delivery.
Rostering is disconnected from care needs and risk triggers.
Service agreements, pricing, and consent records are scattered.
Incidents and escalations are handled well by individuals, but not reliably as a system.
Reporting takes weeks, and leaders can’t see problems until complaints arrive.
And when brokerage expands, the operational cracks widen:
Brokerage handoffs are messy: referrals to partner providers lack consistent scopes, start dates, and documentation expectations; so the client experience becomes fragmented.
Purchase order (PO) control is weak or non-existent: brokered services are commissioned informally (email/text), creating disputes about what was authorised versus delivered.
Supplier invoices don’t match reality: invoices arrive with mismatched client IDs, wrong rates, incorrect dates/times, or extra line items, forcing manual checks.
No clean “3-way match”: without a system linking authorised service (PO) → delivered service (visit evidence/notes) → supplier invoice, finance and operations spend hours chasing exceptions.
Margin leakage: small invoice errors (rate drift, duplicate billing, unapproved add-ons) quietly erode profitability—especially at scale.
Delayed payments strain partnerships: slow dispute resolution damages relationships with subcontractors and reduces availability when you need it most.
This is the scaling trap: as you grow, variability multiplies. You end up with “heroic effort” holding the business together until it doesn’t.
A modern CMS breaks that trap by making the organisation run on repeatable workflows, not personal memory.
How Technology Fixes Brokerage + PO + Invoice Matching (in Practical Terms)
A Support at Home-ready module should treat brokerage like a controlled supply chain, not a loose referral network. Here’s what that looks like.
1) Structured brokerage commissioning (turning referrals into controlled orders)
Instead of emailing “Can you start Mrs Smith next Tuesday?”, the system should create a structured service request:
client + funding stream + goals
authorised service type (e.g., RN visit, physio, transport)
frequency/duration and start/end dates
rate card applied (agreed pricing)
documentation requirements (notes, risk alerts, incidents)
escalation rules (what triggers a call, who to call)
This makes expectations explicit and measurable, and stops “scope creep” before it starts.
2) Purchase orders that mirror care authorisation (POs as the governance backbone)
For brokered providers and suppliers, a CMS should generate POs (or PO-like authorisations) automatically from the care plan/service schedule:
one-off PO for a short episode (e.g., post-discharge RN visits)
recurring PO for ongoing supports (e.g., weekly physio for 12 weeks)
capped values and tolerances (e.g., “no more than X hours/week”)
approval workflows (who authorised, when, and why)
When you scale, PO discipline = control. It’s how you keep financial governance aligned to clinical intent.
3) Delivered service evidence captured once (and usable everywhere)
Invoice matching fails when “delivery” can’t be verified easily. The tech should capture:
delivered visit times (scheduled vs actual)
completion notes (structured, not free-text only)
exceptions (client not home, declined service, worker late)
incident flags (falls, meds, safeguarding)
attachments where relevant (photos for home mods, wound images; where clinically appropriate and consented)
That evidence becomes the “goods receipt” equivalent in a services environment.
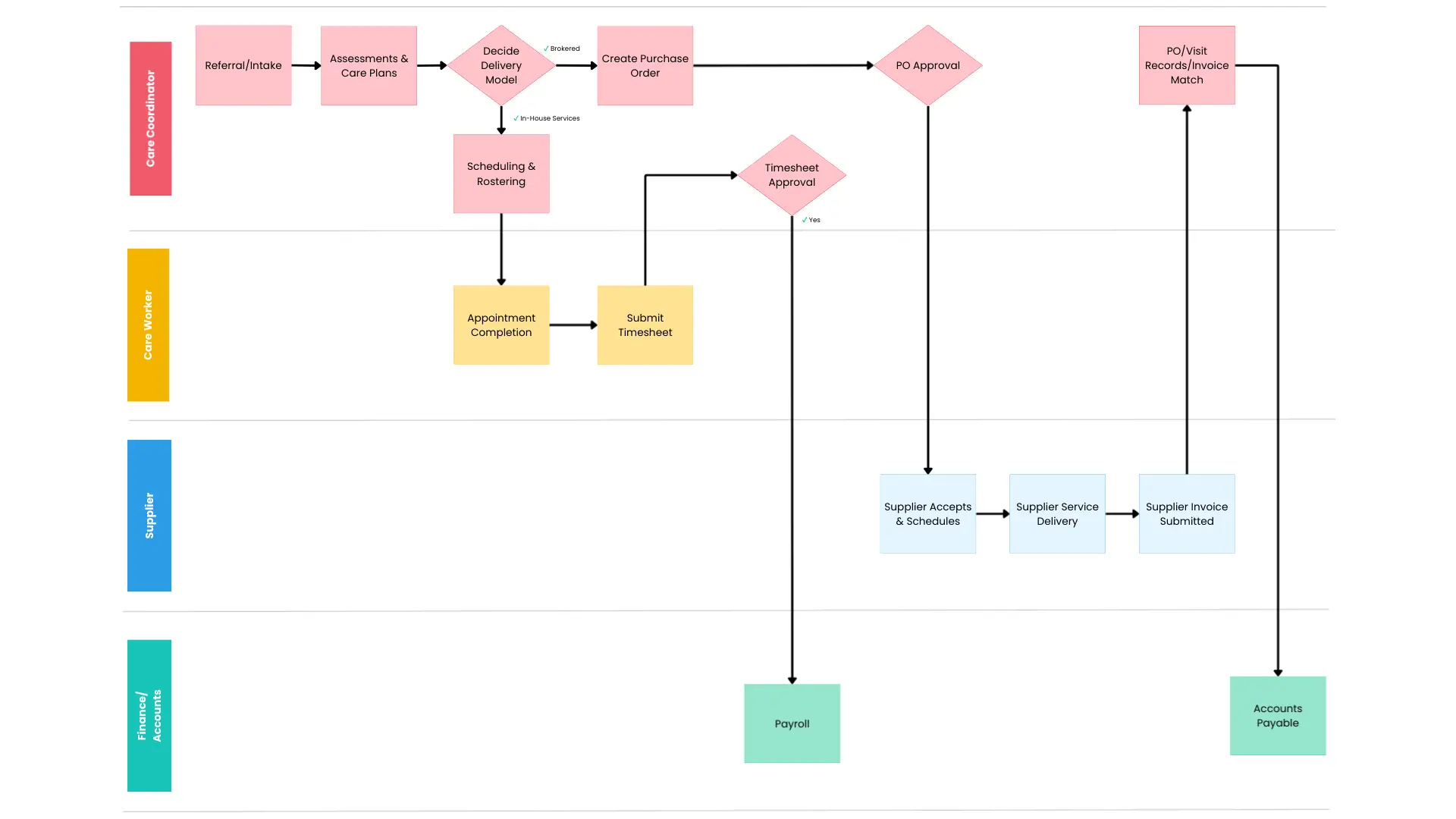
4) Automated supplier invoice matching (the “3-way match” for home care)
The highest-impact feature: automated matching across:
Authorised service (care plan / PO / schedule)
Delivered service (timesheets/visit records/notes)
Supplier invoice (line items, rates, dates)
A robust module should:
match on client, service type, date/time, duration, agreed rate
allow tolerances (e.g., ±10 minutes)
auto-approve clean matches
route exceptions to the right person (operations vs finance vs clinical)
keep an audit trail (what changed, who approved)
This turns invoice processing from a weekly fire drill into a managed workflow.
5) Rate cards + contract controls (preventing “rate drift”)
Brokered suppliers often update pricing, apply weekend loadings incorrectly, or bill at old rates. A CMS should enforce:
supplier-specific rate cards
effective dates (old rate vs new rate)
rule-based loadings (weekends, after-hours)
client-specific variations (if negotiated)
When scaling, the system; not individuals, must be the keeper of “the truth” on pricing.
6) Real-time dashboards for brokerage cost, quality, and risk
You need visibility across the brokered network:
unfilled services / late starts
exception rates by supplier
incident rates by supplier/service type
invoice exceptions by supplier (most common mismatch reasons)
brokerage margin by client/cohort/service
That gives you leverage for supplier performance conversations and smarter panel management.
Where DC2Vue Support at Home Module Fits
A platform like DC2Vue Support at Home Module can support scaling by making brokerage and subcontracted delivery “system-led”:
Care plan as the source of truth (services, frequency, goals, risks)
Orders/POs generated from plan (authorisation, caps, approvals)
Delivery evidence captured against the order (notes, exceptions, incidents)
Supplier invoices matched against authorisation + delivery (auto-approval + exception workflow)
Governance and reporting built-in (audit trails, dashboards, compliance artefacts)
This is what lets providers scale volume without losing control.
Bottom Line: Brokerage Doesn’t Scale on Spreadsheets
Brokerage is a growth lever, but it adds complexity fast. Without strong PO control and invoice matching, providers experience margin leakage, disputes, delayed payments, and fragmented client outcomes. With the right technology, brokerage becomes a controlled, transparent, auditable supply chain: authorise → deliver → verify → pay, all connected back to the client’s plan and goals.
